Estrogen, Progesterone, and Contraceptives in Female Athletes - Episode 50
Feb 07, 2020By request, this topic is both very interesting and very difficult to address for all of the female athletes out there. Studies show that "the female sex steroid hormones estrogen and progesterone have potential effects on exercise capacity and performance..." on top of the very big grain of salt that is bio-individuality. We can study these hormones and learn clinical evidence about how they work and how they may work for or against the female athlete demographic but keeping in mind their unique biochemistry, metabolism, etc. is paramount.
Connect w/ me @jadeteta
Learn more about becoming a Next Level Human at www.jadeteta.com


Jade: [01:17] What’s up, everybody? Welcome to today’s show. This is a show that I’ve been putting off for a long time. It’s actually a request I’ve gotten from someone probably back 4 or 5 months ago, maybe even longer; maybe even 6 or 7 months ago. And it’s a very interesting topic, but a topic that is also very difficult, and this is the topic of estrogen and progesterone related to exercise performance in women, and particularly, oral contraceptives or contraceptive use. Hormone replacement therapies, things like that, and how they impact athletic women. Now, you can imagine, this is one of those areas that is just super touch to understand. Now, obviously, I have a lot of background in this area and spend a lot of time researching this, but especially when you start talking about athletes and exercise performance, this becomes difficult. I’m going to start out this episode by just giving you an idea of reading directly from a study to kind of just give you an idea of how difficult this is. And then, we’ll get into some of the things that I can – I feel like I can say on this subject, but you have to understand, we’re going to have to take all of this with a very big grain of salt, even though hopefully I’ll be able to give you some really useful information here and tackle some of this stuff. But let’s just start with this idea of female athletes and estrogen/progesterone related to contraceptives, and what the research says. So, here’s a quote I took directly from an article that looks at this stuff, a review article that’s looking at this stuff, and it says, “The female sex steroid hormones, estrogen and progesterone, have potential effects on exercise capacity and performance through numerous mechanisms such as substrate metabolism, cardiorespiratory function, thermoregulation, psychological factors, and injuries. Consequently, hormone level changes may theoretically lead to either improved or decreased performance as various times throughout the menstrual cycle. Numerous methodological issues…” you guys know that word, right? “Numerous methodological issues and a paucity of studies have precluded evidence-based conclusions in almost every area of research in this field. In addition, there appears to be a great degree of inter- and intra- individual variability in these hormone responses. Using oral contraceptives may be advantageous for female athletes who are negatively impacted by their menstrual cycles, as they may provide a stable yet controllable hormonal milieu for training and competition.”
[04:01] So, that gives you an idea. Essentially, what they’re saying is look, there’s a lot of research in this area, however, there’s a lot of inter-individual… I don’t know why I can’t talk today – but differences individually and intra-individually, which means there’s differences between women that make comparisons difficult, and there’s even differences within… the woman herself with these changing hormonal relationships that are going on inside a single female’s body throughout the menstrual cycle. With all of that being said, and hopefully I’ll be able to keep my thought process clear, this is – by the way, for those of you who don’t know, it’s funny, I am hypothyroid, so I take my thyroid meds and some days… actually, I took my thyroid meds this morning, but some days when I don’t it’s like my brain is just scattered like this, so hopefully I won’t be fumbling all over my words in today’s episode. But, just keeping it real. We’ll see what happens. Alright, let’s get into this really quickly. First of all, I want to cover for you the differences between estrogen and progesterone. Now, let’s keep in mind, I just read for you that statement, tells you a little bit about the difficulties in making sense of all this information. One of the other areas that’s very difficult for us to make sense of this is the differences between animal studies – rats and humans. Most of the research that we’ve gotten on the differences between estrogen and progesterone come from rat studies. Now, we use mice for a reason when we do studies because their metabolism is pretty damn similar to ours and has been a pretty reliable way for us to test things and then bring them into our clinical practice, and this is true of drugs and everything else. So, using mice as a surrogate for human metabolism works really well. It’s served us pretty well, and that’s why it’s done so often. However, it’s not perfect, so we do always kind of have to say well, that was rat studies, but not necessarily human studies; just ‘cause it showed up in rat studies doesn’t mean it’s true of humans. So, most of what I’m going to talk about is actually in rat studies… although, there is data in humans that I’ll be getting to that as well. Let’s start at the beginning of this. Before we get into oral contraceptives and things like that, let’s get into the differences between estrogen and progesterone. The way I like to conceptualize estrogen and progesterone is as two twin sisters who are nonidentical. So, they’re twins, and the reason I say they’re twins is ‘cause they do have some overlapping functions. They require and are dependent on each other. In other words, estrogen receptors are primed by the hormone progesterone, and progesterone receptors seem to be primed by estrogen. Also, in the hypothalamus, the hypothalamic-pituitary-gonadal axis, or ovarian axis, progesterone and estrogen sort of regulate each other, so throughout a female cycle, if she doesn’t get exposed to the right amount of estrogen, then she may not be able to respond to progesterone correctly, and vice versa. So, that’s why I say these two hormones are twins. Kind of in the way that twins – we tend to think of twins are sort of connected at the hip, so to speak, a little bit closer, a little bit more alike, a little bit more dependent on each other than maybe non-twin siblings. But, they’re not identical. In other words, they don’t do the exact same things even though they’re highly reliant on each other, so that’s why I say estrogen and progesterone are like nonidentical twins. So, if we take these nonidentical twin sisters, we can kind of look at them from the standpoint of one of the sisters, estrogen, is very adventurous, very rambunctious, very resilient.
[08:12] This is the sister that wants to charge out into the world, is courageous, is strong, is sort of – she’s the athlete and the one that can get herself in trouble. She’ll push forward. She’s the one that is like all about taking risks, and working hard in the gym, and she can withstand a lot. If you understand that, this very resilient, courageous, adventurous, out there just attacking life individual, this is what estrogen is like. And this is manifested in the research by the fact that we know, estrogen is kind of like weak testosterone. So, it helps women build muscle. It helps women burn fat. It helps women be a little bit more insulin sensitive. And it definitely blocks the effects of stress. Estrogen is a very potent, powerful… I love this hormone. Of all the hormones that you study, estrogen is my favorite because it just does a ton, a ton of stuff. But, here’s the interesting thing about estrogen – and just to kind of break this down just so we understand – when estrogen is around for a woman, she can tolerate higher amounts of stress, which means she can train harder, and she can train more frequently if she’s an athlete. It also means when we say estrogen makes a woman more insulin sensitive, it means that if she’s in calorie surplus, she’s less likely to store those calories as fat and more likely to build muscle with them. By the same token, if she’s in calorie deficit, she’s more likely to burn fat and less likely to burn muscle. So, estrogen allows a woman to train harder, to recover faster, to build more muscle, to potentially burn more fat, to handle excess stress. This is why we say estrogen – the sister estrogen – is very rambunctious, adventurous, go-getter, because she has a lot of competence and confidence that she can get the job done. Now, progesterone is the opposite of that. Remember, they’re twin sisters, they love each other, so progesterone is trying to look out for estrogen just like estrogen is trying to look out for progesterone. Estrogen is one extreme – rambunctious, adventurous, go out there and attack, do, do, do, build up. Progesterone wants things to calm down. She wants to relax. She wants estrogen not to get in trouble. She wants estrogen to stay at home. She wants estrogen to take a deep breath. She wants estrogen to do yoga instead of lift weights and go out there and do high intensity interval training. She is the calm one, the one that’s always thinking ahead, the one that’s being like oh no, we could get in trouble here, we gotta be careful, and calm, and considerate, and consider our choices. She’s kind of like the parent here, trying to keep them from getting in trouble. If you imagine these two sisters running around together, estrogen’s out there, c’mon, let’s do it, let’s do it, let’s do it, let’s go, let’s go, this is going to be fun, and progesterone’s more like listen, let’s take it easy, let’s be careful, let’s plan this thing out, let’s not get in too much trouble, that could be dangerous. So, this is the way to think about this. Now, when you think about it from that point of view, one place where they do overlap is they definitely help with stress management. Both progesterone and estrogen are anti-cortisol hormones; however, progesterone works against estrogen’s positive impact on insulin. This means when progesterone is around, or her influence is dominating, you’ll tend to not be able to be as stress resistant - she does have some of that capacity, but estrogen is a little bit more so - and you will see that you will not be as insulin sensitive.
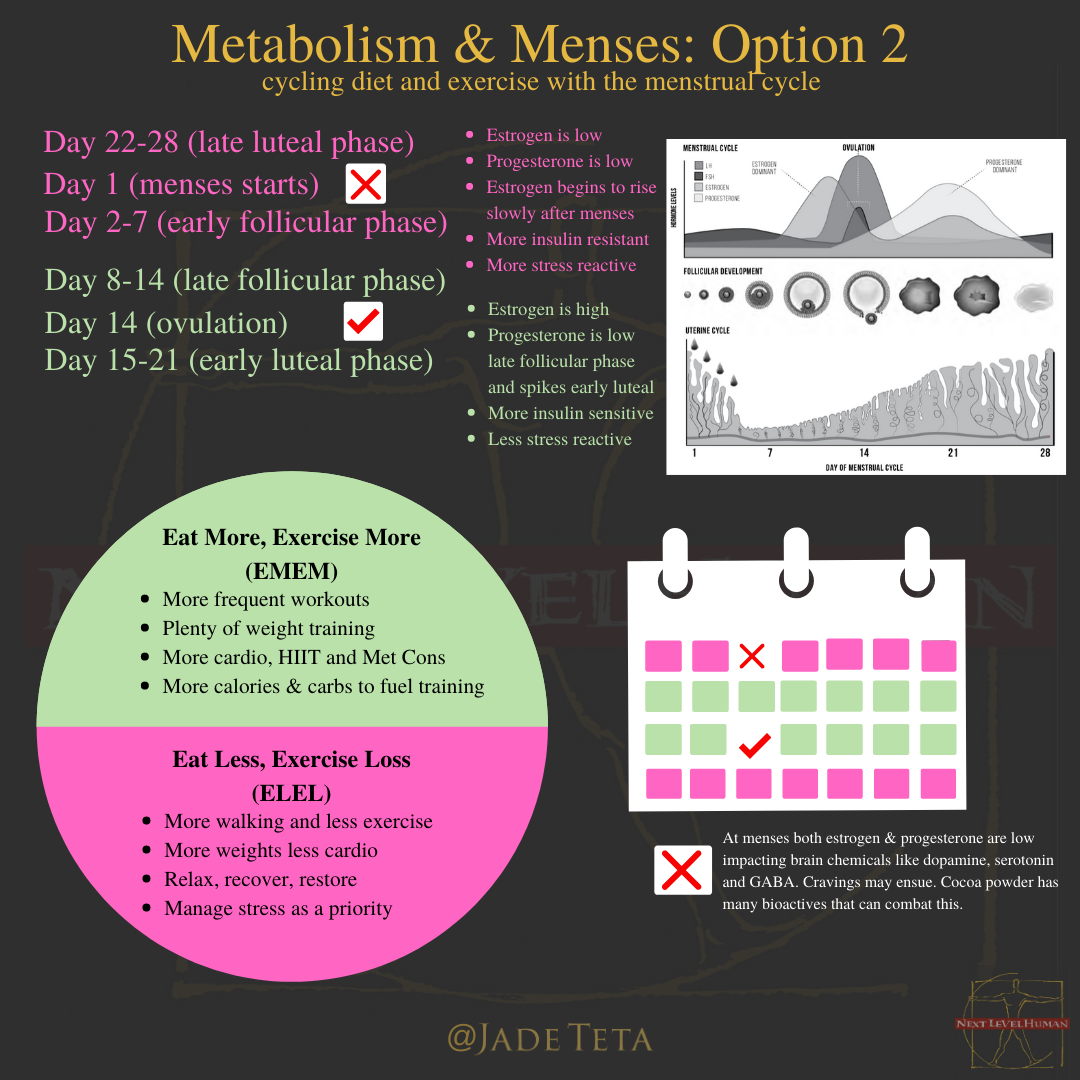
[12:01] Typically when the progesterone sister is kind of in control, you will think that the physiology is going to be less insulin sensitive – or more insulin resistant – and a little less able to handle stress. When we go into the menstrual cycle then, we can break down the menstrual cycle into several different phases, and I want to do this first before we start talking about athletes, just so we’re all clear on this. The menstrual cycle can really be broken down into two phases… and I’ll slow down here because this can get really confusing, and it has to do with talking about estrogen and progesterone and their relationship, relatively speaking vs. absolutely speaking. For example, you can have absolutely high amounts of estrogen, but it can still be relatively less than progesterone if progesterone is higher. So, I’ll walk you through this and hopefully this will make sense. Let’s go through the simple version first. At the beginning of the menstrual cycle, day 1 of bleeding, that’s the first day of menses in a cycle. For the first two weeks roughly… remember what happens at menses – the uterine lining is shedding, hormone levels are very low, estrogen and progesterone are both very low at day 1. And then, what happens is, under the influence of follicle stimulation hormone, FSH, coming from the pituitary gland, the ovaries begin to ramp up their production of estrogen. So, estrogen levels are low at the beginning of the cycle. After about 4 or 5 days, halfway through that first week, estrogen levels start to rise. By the time you get into that 2nd week, estrogen levels are getting higher. So, for that first 2 weeks, you have sort of this slow rise in estrogen the first week, and then estrogen starts to get high in the 2nd week. Now, what’s interesting here is in this first 2 weeks of the menstrual cycle, progesterone is essentially nonexistent. That sister is basically at home lying bed not out playing. Estrogen is out playing by herself, and potentially out there playing and doing things. She’s got free rein, right? So, progesterone is not around. As a matter of fact, the first two weeks of the menstrual cycle, progesterone is absent essentially. Women have the same amount of progesterone, roughly speaking, as a man would during the first half of the menstrual cycle. So, the estrogen sister plays alone. First, she just ramps up, and then she’s high in the second. We call this the follicular phase of the menstrual cycle. We call it the follicular phase of the menstrual cycle because follicle stimulating hormone and the development of the follicle is ramping up, so we basically say that the follicle, which contains the egg, is maturing during the follicular phase. And as it matures, estrogen levels become higher and higher and higher. After about two weeks of that, you get ovulation occurring. This happens once the estrogen levels sort of reach a peak, and the hypothalamus sort of gets the signal between the relationship between estrogen and FSH and another hormone called LH, luteinizing hormone, and luteinizing hormone will spike right around the ovulation time, and that causes – or is correlated with – the rupture of the follicle and the release of the egg. So, right here in ovulation, the follicular phase of the menstrual cycle ends, and the luteal phase begins to start. They call it the luteal phase because it is triggered by the luteinizing hormone. Also, once that follicle ruptures and the egg is released, that follicle then becomes the corpus luteum, and the corpus luteum becomes the source of progesterone. So, in the 2nd half of the menstrual cycle, you start getting progesterone levels rising.
[16:00] Now, what’s interesting about this is that estrogen levels don’t necessarily fall off right away; they still remain higher, it’s just that now it’s playing with progesterone. So, progesterone starts to exert influence. Now, at the beginning of the luteal phase, estrogen is still dominating a little bit, so it’s still high there, but progesterone starts to dominate. And by a few days, progesterone is starting to dominate a little bit. The point is, during the follicular phase, estrogen is playing by herself, and then the luteal phase, estrogen and progesterone are playing together, especially in the early luteal phase, the beginning of the luteal phase, and that’s the next way we can think about this. But at the end of the luteal phase, both estrogen and progesterone fall off if the egg does not get fertilized, and you get this sharp drop in both estrogen and progesterone. Estrogen first, progesterone second. Then, you get lack of estrogen and progesterone influence on the uterine lining, and the uterine lining degrades and sheds, and you get bleeding and the whole thing starts over again. So, that’s the simple way to look at the menstrual cycle, as a follicular phase where estrogen is playing by herself, and a luteal phase where estrogen and progesterone are playing together. Now, the more complicated way to look at the menstrual cycle would be early follicular phase, late follicular phase, then early luteal phase, and late luteal phase. Early follicular phase would be the week of menses. The truth here is this is a time of relatively low hormone. Progesterone’s essentially very low and estrogen is rising during this early follicular phase. Now, in the late follicular phase, the week before ovulation, the week after menses and the week before ovulation, you have estrogen rising, progesterone low. So, estrogen is sort of very dominant at this time. Then, you go into ovulation and you move into early luteal phase. In early luteal phase, you have estrogen and progesterone playing together. So, estrogen is high, progesterone is high. Then, you got late luteal phase, where estrogen falls off, followed by progesterone, and then menses starts. So, this is where the complication comes in, because if you look at this from a two phases of the menstrual cycle, follicular phase vs. luteal phase, you’ll see that in the follicular phase, estrogen dominates, relatively speaking, because progesterone’s not around. But in the luteal phase, progesterone dominates, relatively speaking, even though estrogen is still around. This will make sense in a little bit as we start talking about how this works in some of the athletic research. It’s important to understand that in the luteal phase, especially in the early luteal phase, estrogen is still high. Her dominance is still being really felt. Then, late luteal phase, estrogen falls away and progesterone falls away. So, from an absolute perspective, if we look at the menstrual cycle from an absolute perspective, especially as it is related to estrogen, which is the most important sister when we talk about athletic sort of stuff, because we really want her influence. She is going to dominate during the late follicular phase and the early luteal phase. This is important when you start looking at research, because when you look at research on this, it gets confusing because sometimes it’ll say there’s increased performance in the follicular phase, and other times it’ll say there’s increased performance in the luteal phase. And what seems to be the case is that what they’re doing in this research is they’re not distinguishing between the late follicular phase and the early luteal phase, because almost always when you look, that’s going to be the time when estrogen is dominating, which will be late follicular/early luteal. So, I know that’s relatively complicated. I will include an infographic on my site under this episode so you can go and look, that will show you both ways to look at the menstrual cycle in that sort of regard, but this important.
[20:11] So, now let’s get into some of the research on sort of athletic women, and estrogen and progesterone in general. When we look at mainly – this is in rats, because I just told you in the beginning of this how difficult it is to really tease this all out – but right now it looks like, “looks like”, and we have to put this in major quotes and with a huge grain of salt, it looks like that estrogen is the hormone of female prowess in the athletic space. In other words, when estrogen is around, women tend to perform better in terms of their athletic performance… especially as it pertains to endurance type events. This is because it looks like estrogen spares glycogen and enhances fat burning in exercise. As matter of fact, we know in human studies that women burn more fat at all exercise intensities, whether they’re walking or sprinting, than men do, relatively speaking, probably because of the influence of estrogen. We also know that if we give men, exercising men, estrogen, we’ve seen studies where their respiratory exchange ratio goes down. For those of you that don’t know what the respiratory exchange ratio is, it’s just the amount of carbohydrates you burn relative to oxygen; it’s a combination of looking at CO2 vs. O2, O2 being correlated with fat burning, and CO2 being correlated with carbohydrate burning, so this is one way we can measure how people burn fuel during exercise. What we know, that if you give estrogen to men even, their O2 consumption will go up, they’ll use more fat than they normally would. Men tend to be, in general – tend to be, because they don’t have as much estrogen – they tend to be more glycolytic in their exercise. They tend to burn more carbs whereas women burn more fat in exercise. Because of the glycolytic nature, men can really increase intensity and power and strength a little bit more, where women lean more towards endurance because they burn more fat; part of the reason men get more of an afterburn with exercise too compared to women. There’s a lot that goes on here because, obviously, men have more muscle mass as well, but this is part of the way to look at it. So, estrogen is a really important hormone, and it’s the one that we want to look at. As a matter of fact, we typically look at progesterone related to estrogen just how progesterone blocks some of estrogen’s impacts. So, we’re really looking at estrogen here. It’s a really important sort of point to drive home. What the research essentially shows us is that estrogen helps women burn more fat all exercise intensities, helps them spare glycogen, helps them recover faster it looks like, and helps them sort of build muscle and that kind of stuff as well. This is an important consideration here. By the way, when you think about estrogen and progesterone through the menstrual cycle, and if you really want to understand why this is the way it is, think about it this way – the whole point of metabolism is to keep the system balanced. And why would it do that? It’s trying to help you survive any kind of environmental sort of situation so that it can reproduce. So, the major sort of primary thing that the metabolism’s trying to do is reproduction. If you think about the first 2 weeks prior to the egg being released of the menstrual cycle with estrogen being around, this is really about building up tissue. This is about getting stronger, building up, you know, helping fat storage and muscle storage and all that kind of stuff. And being able to build up and adapt faster. Get stronger, basically.
[24:01] But once the egg is released and is potentially going to get fertilized, it’s really useful for the metabolism to conserve fuel, especially because it now might need to feed two people: one, the mom, and two, the fetus. And this is one of the reasons why the female metabolism gets more insulin resistance post-ovulation. Because that would make sense, wouldn’t it? Insulin resistance essentially means let’s resist the propensity to shuttle all this sugar and all this fat into our cells, let’s leave some of it hanging out in our blood. The hallmark of insulin resistance is higher blood sugars and higher blood triglycerides, or blood fats. That would make sense to leave that be the case, especially if there was a fetus coming along that needed some of that. So, it was a way for maybe females to provide fuel to this growing fetus. Hopefully that makes sense. Estrogen building up, adaptation, progesterone taking it easy, saving fuel for a potentially coming baby. That also should give you a little bit of sort of understanding about what happen through exercise performance, that it would make the most sense that exercise performance, in terms of the ability to burn fat and maybe endurance types of things, would be better when estrogen is higher in absolute amounts. This would be right around ovulation. This would be the week before and the week after ovulation, right in the middle of the cycle when estrogen is higher. Then, estrogen drops off, then followed by progesterone in the late luteal phase, and then menses, both are relatively low with estrogen rising. So, you can kind of think of this as the week before menses and the week during menses females are more like a male metabolism. What you’ll see is they become a little bit more insulin resistant, a little bit more reliant on carbohydrate for energy, a little less reliant on fat for energy, and they become a little bit more carbohydrate burners. They become better at burning carbs, worse at burning fat, much like a male vs. the middle of the menstrual cycle, it would make sense they’re a little bit more endurance. So, this can give you sort of when would you want to go for a PR in resistance training or a sprint. Maybe, and some research hints at this – when I say hints, again, a very big grain of salt, this may be the case – but some research hints that if you’re doing high intensity strength and sprint-based stuff, you might want to do that around the menstrual cycle, the week before and during the menstrual cycle. However, if you’re going to run a marathon or do something that has a lot of endurance and relies on a lot of fat, you might want to do that in the middle of the menstrual cycle if you’re tracking this. Hopefully that begins to make some sense. Now, the question is, and the whole request for this particular episode, was really about well, what about contraceptives. Now, contraceptives – you think it’s complicated now, it gets even more complicated, which is why I put this off for so long in terms of doing this particular episode. But, I know a lot of you are very savvy, and hopefully you’re following me, and you can listen to this over and over and over again. Here’s the interesting thing with contraceptives – contraceptives are essentially ethinyl estradiol, which is not estrogen. It works like estrogen – it’s essentially horse estrogen. It is a estrogen that acts like our estrogen in most ways, but is weaker in some ways and much stronger in some ways in terms of its impact. It’s useful to remember, there are receptors for estrogen all over the body. In the uterus, yes, in the ovaries, yes, in the breasts, yes, but also in the muscles, and in the brain, and the fat tissue, the adipose tissue. So, ethinyl estradiol is going to interact with these receptors. It’s not exactly the same as a woman’s normal estrogen, and so it can act weaker or more strongly in certain areas.
[28:06] The other thing to understand is when oral contraceptives first came out, they were given very high doses of these. The amount of ethinyl estradiol in oral contraceptives now is much, much less. I think it’s only 1/3 of what it used to be, which decreased some of the risks; but one of the risks with estrogen in general, whether you’re taking bioidentical estrogen or ethinyl estradiol orally, whenever you take those hormones orally, because they have to go through first pass in the liver, they are correlated with increased clotting factors being produced in the liver, which is why they have some negative association with cardiovascular disease and clotting. This is definitely something that is an issue that you probably heard about from your doctor if you’ve gone on oral contraceptives. They’ve gotten much safer because the estrogen is much, much less. This also gives any of you women who are perimenopausal or menopausal, it’s also the reason why natural medicine practitioners hardly ever use a bioidentical oral estrogen. We typically use transdermal estrogen to avoid this first pass and the coagulation issues with oral estrogen. Now, same thing with progesterone. Oral contraceptives are not bioidentical progesterone, they’re progestin. And this is where is gets very, very complicated because there are many, many, many different compounds, drugs, that are progestins that, again, act like progesterone in sort of the main ways to trick the body into thinking it’s in a luteal phase, thinking that the egg has already been released. But also, they can have many, many factors on all the other areas that progesterone would impact: skin, ovaries, breasts, uterus, brain, muscle, all these other organs, So, what we now know is that certain progestins have certain effects. Some progestins can have weak estrogen effects. Some progestins can be weaker or stronger in their progesterone effects. Some progestins can have androgen-like effects, and this is something that I have put also a resource for that I’ll leave with this particular episode as well that gives you an idea of some of these progestins. Again, another big caveat here, we don’t know a lot about this and almost no physicians understand this, and I’ll tell you what this was like. I was seeing all these different progestins doing different things, and even I don’t know this. If you were like hey Jade, what does norgesterone do, or what does this particular progestin do, I would have to go look that up because I don’t have that stuff memorized. There’s just too many of them. There’s just way too many of them, so we really don’t know, but suffice it to say, this is why this gets so complicated. Because you got ethinyl estradiol, it’s not like your normal estrogen. Then, you got all these different progestins - and I have put together a resource for you to go and look, where you can go what oral contraceptive am I on, is it ethinyl estradiol plus which progestin, and then I have a chart where you can go and look at the progestin and see some of the effects, and some of those things may or may not be good. For example, if you’re someone who deals with acne, you wouldn’t want to go on an oral contraceptive that has a progestin that is more androgenic in nature. As a matter of fact, you’d want to go on a progestin that is less androgenic in nature. A lot of times, your doctor just prescribes whatever their favorite one is, or whatever the recent pharmaceutical rep told them about, versus understanding which of these things impact like that, so this is really useful for you to do. But the point is this – how does this impact athletic females? Well, here’s an interesting thing - what exactly does oral contraceptives do? Well, what they do is they take this cycle away. Remember when we talked about the follicular phase vs. the luteal phase, and how the luteal phase comes after ovulation? Once the egg is released from the follicle and it becomes the corpus luteum, the hypothalamus is reading that stuff.
[32:02] Remember, the metabolism is like a thermostat, so the hypothalamus is reading that and goes oh, an egg has been released, you don’t need to release another one. So, if that luteal phase hormonal situation stays permanently, then the brain keeps getting the signal that the egg has been released and it never goes back through the cycle again, and that’s how oral contraceptives work. They put you in a constant luteal phase. They basically put you in a late luteal phase, where you have estrogen and progesterone, but with progesterone dominating. This is also one of the reasons why you actually don’t need estrogen in these oral contraceptive pills, and that’s why some will just be progestin only oral contraceptive pills. So, this is what is happening here, it’s putting women in a luteal phase. When you look at it from that point of view, you go oh, well, these put you in a state where it looks like you may be best off for sort of this endurance effect. Estrogen is high, progesterone is high, and you can get some good effects here. As a matter of fact, what they see with oral contraceptives and hormone replacement therapy in menopause is that metabolic rate is upregulated. That’s not necessarily a great thing, by the way. A lot of people hear that and they go, well, that means they cause weight loss, but anytime you upregulate metabolic rate, you also tend to upregulate hunger. This is why you see people who go on oral contraceptives, women, some of them gain weight, some of them lose weight, most of them stay the same. That’s also why the research is sort of not clear on this because certain people are going to be sensitive to this upregulation and appetite, or not. Imagine you’re a person who’s not sensitive to this upregulation and appetite, you start taking oral contraceptive pills, your metabolic rate goes up, you don’t respond with increased hunger, you might lose weight. Let’s say though you’re someone who this metabolic rate stimulation goes up and you overcompensate with increased hunger, you will actually end up gaining weight. So, this is part of the issue here. But, the point is, the whole point of this particular podcast is what do we do about oral contraceptives with female athletes? Well, interestingly enough, let’s say you’re a female athlete that is… you might notice that in certain months of the menstrual cycle you perform better than others, or you just – I’ve heard some women say, actually surprisingly enough, during menses, I perform best. This may go right along with – I have never correlated with are they sort of anaerobic type athletes, sprinters, and weightlifters, stuff like that. Probably, because that’s mostly who I spend my time with. I don’t spend my time with a lot of endurance athletes. But, that would make sense that they would maybe do their best around menses and those particular sports. But the point here is that if we take this standard oral contraceptive, it’s putting you in sort of early luteal phase for most women. So, that is an interesting thing, and may actually be beneficial for women. Now, if you’re a woman who feels like I know that my performance varies and sometimes it’s really bad, and I can’t predict when, you know – let’s say I’m an endurance runner, I run track, I run something like in between. I’m not a 100m dash runner and I’m not a 5k runner, I run the 400m, and I notice that around different types of my cycle, I perform better or worse. This may be a useful thing to do. Oral contraceptives, one of the benefits might be that it’ll smooth this whole thing out, especially the monophasic oral contraceptives, which is one dose of oral contraceptive across the board would probably be, or might be, a good idea for that particular woman. And she may opt one, to stay on oral contraceptive pills, or to go on oral contraceptive pills, and also to opt out of the placebo week. The placebo week is basically something that oral contraceptive companies will give you just to induce menses, but you don’t have to.
[36:08] You don’t have to take those placebos to get menses. A lot of times they do that simply because women are used to bleeding and they don’t necessarily want to build up your iron levels, and there’s some benefit to potentially having that monthly bleed. But for athletes, they may want to avoid that, so they may want to go on a monophasic oral contraceptive that keeps them in that late luteal phase so everything is predictable, and maybe opt out of the placebo week so they don’t get menses at all. This would potentially be beneficial to an athletic female. So, again, we have to take a lot of these things with a grain of salt, especially the stuff I’m talking about with a premenstrual and menstrual weeks being better for anaerobic athletes. But, you may want to try that. It makes good sense, and I feel like the research hints that, but we can’t say that for sure; versus the endurance athletes might do better by staying right around a pre-ovulation and post-ovulation weeks for their sports. But let’s face it, not everyone can do that, especially if you’re a college athlete or professional athlete who is essentially needing to… you don’t get to plan your events and games around your menstrual cycle. Hopefully that makes some sense there. A couple other things about this. One of the interesting things about this is that you might say, well Jade, what about sort of progestin only pills, and what about sort of IUDs and things like that? Well, IUDs may be some of the best of all worlds in a sense, but IUDs typically… they are mainly local. Now, we do know, despite what the marketing is, is that these things probably do cross into the blood, and you do get smaller amounts, but IUDs may be even better in terms of how they impact women and athletes, because it’s essentially inserted once and then it’s sort of set it and forget it. These things can also stabilize sort of the hormonal system as well. So, when you’re thinking about this from an athletic point of view, and I won’t ramble on, that was just to give you all the information here, because in the end, the recommendations are pretty simple. It essentially goes like this: if you’re an athletic woman who’s worried about training with the menstrual cycle, and you’re not competing and you’re just thinking of hey, I want to train with my menstrual cycle and potentially use these changes in estrogen and progesterone to, you know, potentially gain muscle and burn fat, and sort of just cycle my diet to keep my metabolism guessing – what you may want to do is periodize your workouts to do the most intense type of stuff and the most muscle building when estrogen is more absolutely high. This would be pre- and post-ovulation, so this is where you might want to do lots and lots of high volume, high intensity, high frequency, lots of cardio, lots of weight training, lots of everything during this time; and that, perhaps, you want to take it easy around pre-menstrual and menstrual. Now, you also could do it where estrogen is relatively higher where you go, well, the first weeks of the menstrual cycle, I’ll spend more time training a lot, and eating more, and all that kind of stuff, and then the second half, the luteal phase, I’ll cut down calories and take it easy. Either one of those approaches will work. If you’re just sort of someone who’s not really an athlete, just trying to lose weight and want this simple, I typically recommend during the first 2 weeks of the menstrual cycle, this is where you’ll train more and eat more; and during the last 2 weeks of the menstrual cycle, this is where you’ll train less and eat less.
[40:02] Now, if you’re more of an athlete, what you probably want to do is put you’re training, and amplify your training, right in the middle of the menstrual cycle pre- and post-ovulation, and leave pre-menses and menses to kind of take it easy and recover a little bit. Hopefully that makes sense. Now, if you’re someone who’s not able to do this and you’re more of a serious athlete, you’re on a sports team and you can’t predict what you do, then yes, oral contraceptives may be beneficial. Would I recommend them? No. I would recommend you stay natural and just look at your menstrual cycle, and deal with that. You don’t need to worry about this. However, many women are on them, or are having difficulty with menses in general, which is the major reason why people go on this now. Many people go on for birth control, but these things are prescribed – don’t quote me on this – but they’re prescribed probably more often, is my guess, for symptom management. There are lots of people on this. As a matter of fact, 82% - somewhere in the 80%, I think that quote is right – 82% of women between the ages of 20 and 35, I believe, are on birth control. It’s some crazy number. I’m not sure if I have that right, but there’s a lot of women on birth control, let’s just put it that way. So, there’s a lot of women on it for some reasons and they’re concerned about it. For athletes in particular, they want to know, is this negatively impacting my training. Probably not, and it can have some benefits in doing things a little bit more predictable. Same token, if you’re not on them and it’s not bothering you, you don’t necessarily need to go on them. By the way, just briefly, risks associated with oral contraceptives – there is a slight increased risk of clotting. That has gone down significantly. There is a slight increased risk of cardiovascular disease because of that clotting sort of effect. And there is some indication that it’s a very small – there was one study that showed a very small increased risk of potential breast cancers, although that looks like that is very controversial as well and probably is not the case. The reason why we say that is probably has to do with progestins and stuff, and they’ve gotten slightly better on this. If you wanted my bias, I’m kind of anti. I would prefer people doing it naturally, but certainly, I don’t think you need to be scared of these particular things. I think that gives you sort of the take on oral contraceptives and how that works and gives you a lot to think about in terms of what these things are doing. I think using them smartly, and hopefully this podcast gives you the ability to think about how I might use them. I don’t necessarily think you need to go off them. For some women, they may choose to go on them, and hopefully you kind of understand how to regulate your menstrual cycle with training either way with this. So, hopefully you followed me on this. I know this podcast is kind of feels all over the place. That’s because the research is all over the place. But hopefully I gave you some good to-dos, and I’ll go through those one more time just so you have them. So, there’s two ways to look at the menstrual cycle – you can look at it as two phases, follicular and luteal phase. If you’re going to look at it that way, and you’re just a regular training woman who’s trying to optimize body composition, eating more and exercising more might do better in the follicular phase because estrogen is dominating. Sort of eating less and taking it easy might work better in the luteal phase because progesterone is dominating. Now, if you’re more athletically inclined, a CrossFitter, someone like that, who’s doing recreational competitions and is not super serious about this but does potentially want an advantage, you may want to try scheduling some of your PRs and things like that around pre-menstrual and menstrual when you’re more like a male in your physiology, and you’re more anaerobic in nature and glucose dependent. And you may want to run your 5ks and marathons and things like that during the pre-ovulation and post-ovulation period when estrogen is sort of much, much higher.
[44:11] So, hopefully that makes sense. Now, as far as oral contraceptives, they put you in a luteal phase, so they make you a little bit more like early luteal phase; so estrogen is high and progesterone’s high if you’re doing a mixed estrogen/progesterone OC, oral contraceptive. If you’re doing a progesterone only one, then that looks a lot like late luteal phase. So, there are some differences there, but the benefit of that would be just smoothing out the rhythm so you don’t have to have it. So, if you’re an athlete who has lots of pre-menstrual issues, it interrupts training, the bleeding is bothersome and inconvenient, and you went on oral contraceptives for that reason and you’re worried about being on them, they actually don’t have any negative impact that we can see, and the research on training, it may actually provide some benefit for some women, depending on the formulation that you’re using, so they tend to be a good choice. Now, if you’re someone who wants sort of less risk and even less hassle, then you could go with the IUDs, and this could be a good way to do this as well. Hopefully that gives you a lot of things to think about. Go check out the resources on my site. Just go to jadeteta.com, hit on podcasts, go to this podcast episode, which I think – let me just go to my device and I’ll give you what this episode is going to be – I believe it is going to be… I think it’s episode 50. Yep, this is episode 50, so you can just go to my website, www.jadeteta.com, podcast, episode 50, and there’ll be some resources there for you, probably by the time this goes live. I’m going to stop right there. Hopefully you followed me today, and I will talk to you at the next podcast. Thank you so much everybody.
Stay connected with news and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.
We hate SPAM. We will never sell your information, for any reason.
